

A scoliosis is a lateral curve in the spine. This means that when viewed from behind, the spine is not completely straight. It is not to be confused with kyphosis or lordosis. These are anterior-posterior curves and they are completely normal. You have a kyphosis where your upper back sticks out, and lordoses at the neck and lower back.
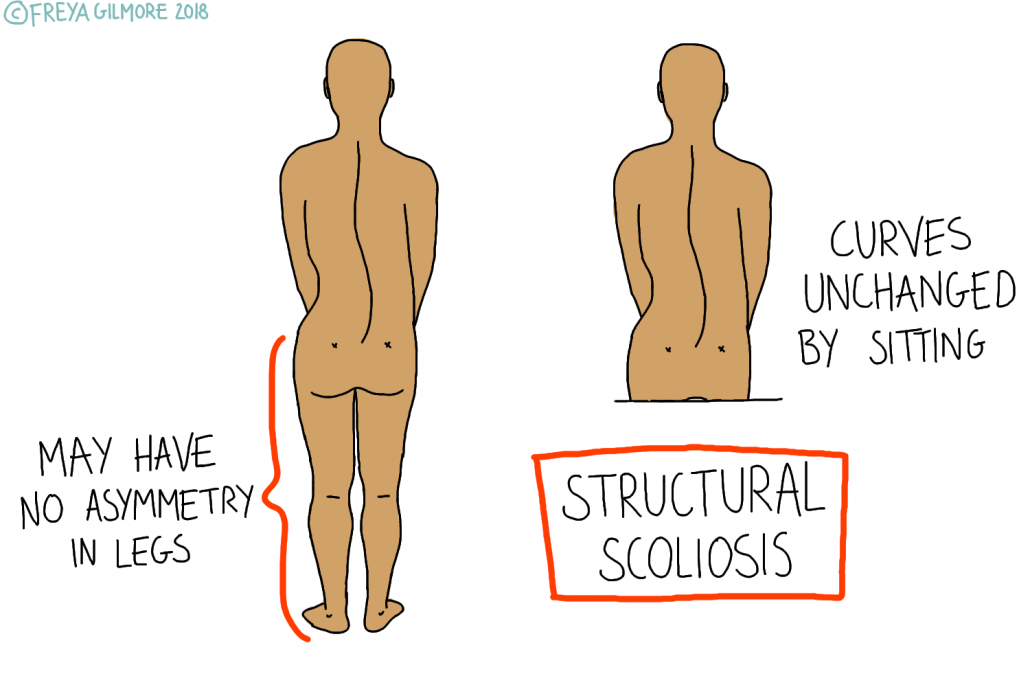
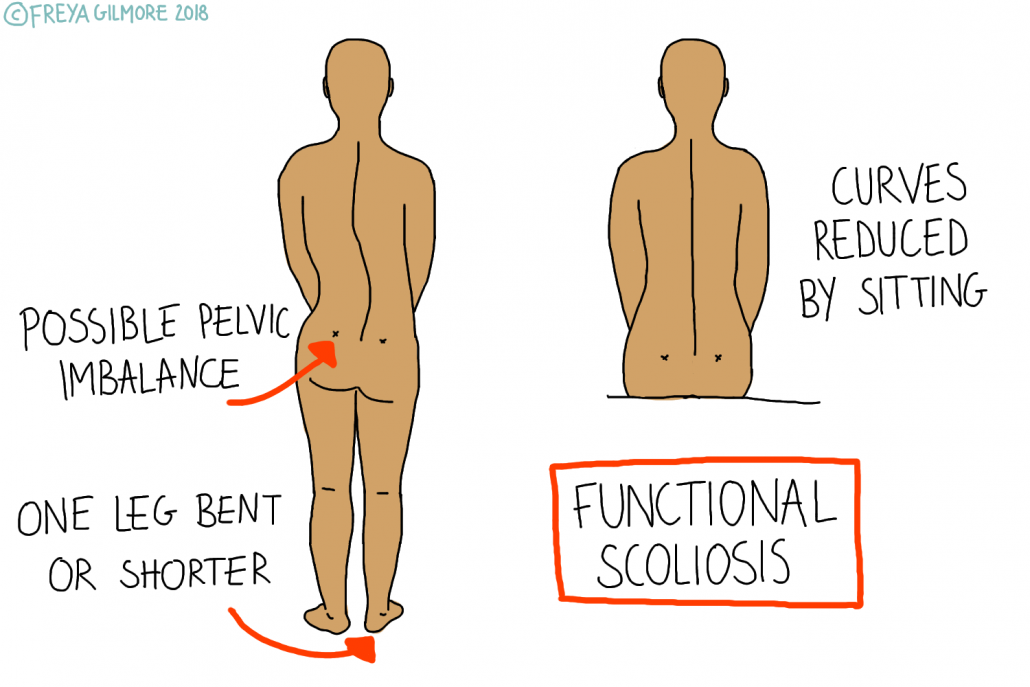
Most people have some degree of asymmetry, and there is no minimum size to define a scoliosis. However, severity dictates the intervention that would be offered, and to some extent, the symptoms associated. A true scoliosis is often initiated by an unknown cause, often in adolescence and occasionally in infancy. A positional (or “functional”) scoliosis is only present in certain positions: often it disappears when sitting.
Is it Serious?
Scolioses are mostly idiopathic: we don’t know what causes them. Sometimes they are associated with other conditions, including genetic conditions like Marfan’s Syndrome and Ehlers Danlos. They might also appear alongside cerebral palsy or some forms of muscular dystrophy. However, 80% are unrelated to another condition. New cases should be seen by a GP to ensure the correct pathway is taken.
The severity of the condition is measured based on an X-Ray. From an image of the spine from the front or back, lines can be drawn to find an angle. This number gives an objective measure that can be used to determine the next steps. It is recommended that mild cases are managed conservatively, such as with manual therapy and exercise. Intermediate cases in adolescents may respond to a back brace. The most severe cases may be candidates for surgery.
Transient Scoliosis
The most mild scolioses are transient. A functional scoliosis is often caused by a leg length discrepancy. Again, most people are slightly asymmetrical, so this is not uncommon. Most people are likely to be asymptomatic, but others may develop lower or upper back pain. If you stand with one hip higher than the other due to leg length, the body will correct itself on the way up. It wants your eyes and ears to be level, so it compensates for the curve within the back. This often causes an “s” shaped curve while standing, which may mean one shoulder is higher than the other too. As with other scolioses, there may be some rotation through the back too, which could impact the ribs and cause aches and pains associated with that. Because the cause is below the pelvis, curves resolve when the person sits down.
Similarly, an antalgic posture can cause a temporary scoliosis. This is a posture in response to pain, which we commonly see in clinic. Lower back pain can often cause an antalgic posture, sometimes encouraging the patient to lean away from the cause of pain. When the pain is resolved, the posture corrects itself too.
Osteopathy for Scoliosis
We cannot cure a true scoliosis, but we may be able to help provide some relief. Pain can come from muscular tension, as some muscles are constantly stretched, and others are contracted. By helping to relax and strengthen these muscles, a patient may find some comfort. The rotation that typically comes with the curve can compress the ribs too, affecting the joints at the spine and the diaphragm muscle. When the diaphragm is impacted, the smaller muscles around the neck and shoulder have to work harder, becoming fatigued and sore. Improving the breathing mechanics can have positive repercussions throughout the body.